


Symptoms, Causes, Diagnosis, and Treatment of Ovarian cysts - Adnexal Cyst and Mass
An adnexal mass, or adnexal cyst, is a growth that occurs in or near the organs attached to the uterus in women. This is what is called the adnexa region and includes the fallopian tubes, ovaries, uterus, and the connecting tissues.
Women of all ages may develop an adnexal mass, especially in the ovaries.
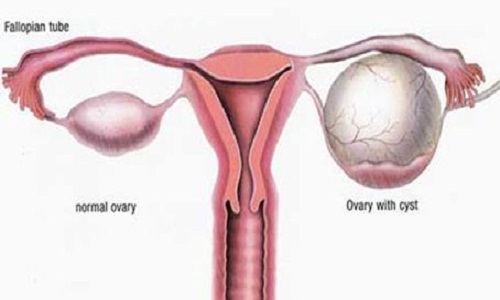
Ovarian cysts are fluid-filled sacs or pockets in an ovary or on its surface. Women have two ovaries — each about the size and shape of an almond — on each side of the uterus. Eggs (ova), which develop and mature in the ovaries, are released in monthly cycles during the childbearing years.
Many women have ovarian cysts at some time. Most ovarian cysts present little or no discomfort and are harmless. The majority disappears without treatment within a few months.
However, ovarian cysts — especially those that have ruptured — can cause serious symptoms. To protect your health, get regular pelvic exams and know the symptoms that can signal a potentially serious problem.
Women aged 40 and above with an adnexal cyst or mass have a greater chance of developing ovarian cancer.
What are ovarian cysts?
The ovaries are part of the female reproductive system. They’re located in the lower abdomen on both sides of the uterus. Women have two ovaries that produce eggs as well as the hormones estrogen and progesterone.
Sometimes, a fluid-filled sac called a cyst will develop on one of the ovaries. Many women will develop at least one cyst during their lifetime. In most cases, cysts are painless and cause no symptoms.
Types of ovarian cysts
There are various types of ovarian cysts, such as dermoid cysts and endometrioma cysts. However, functional cysts are the most common type. The two types of functional cysts include follicle and corpus luteum cysts.
- Follicle cyst
During a woman’s menstrual cycle, an egg grows in a sac called a follicle. This sac is located inside the ovaries. In most cases, this follicle or sac breaks open and releases an egg. But if the follicle doesn’t break open, the fluid inside the follicle can form a cyst on the ovary. -
Corpus luteum cysts
Follicle sacs typically dissolve after releasing an egg. But if the sac doesn’t dissolve and the opening of the follicle seals, additional fluid can develop inside the sac, and this accumulation of fluid causes a corpus luteum cyst.Other types of ovarian cysts include:
- dermoid cysts: sac-like growths on the ovaries that can contain hair, fat, and other tissue
- cystadenomas: noncancerous growths that can develop on the outer surface of the ovaries
- endometriomas: tissues that normally grow inside the uterus can develop outside the uterus and attach to the ovaries, resulting in a cyst
Some women develop a condition called polycystic ovary syndrome. This condition means the ovaries contain a large number of small cysts. It can cause the ovaries to enlarge. If left untreated, polycystic ovaries can cause infertility.
Symptoms
Some women with the condition will not experience adnexal cyst symptoms while being unaware an adnexal mass growth is even present. It is through a routine pelvic exam that an adnexal mass is typically discovered.
In some cases, adnexal cyst symptoms will occur, but this depends largely on the size of the mass.
- Pain or pressure in the pelvic region
- Abdominal distension
- Constipation and gastrointestinal disorders
- Bleeding at the site of the cyst or mass
- Back pain
- Irregular periods in women experiencing pre-menopause
- Difficulty with urination
- Frequent urination
- nausea and vomiting
When to see a docto
Seek immediate medical attention if you have:
- Sudden, severe abdominal or pelvic pain
- Pain with fever or vomiting
Causes
There are a variety of different adnexal cysts and masses. Some fluid-filled growths arise in the woman’s ovaries; others have both solid and liquid matter (called septated) and are especially dangerous.
Most cysts develop as a result of your menstrual cycle (functional cysts). Other types of cysts are much less common.
Functional cysts
Your ovaries normally grow cyst-like structures called follicles each month. Follicles produce the hormones estrogen and progesterone and release an egg when you ovulate.
If a normal monthly follicle keeps growing, it's known as a functional cyst. There are two types of functional cysts:
- Follicular cyst. Around the midpoint of your menstrual cycle, an egg bursts out of its follicle and travels down the fallopian tube. A follicular cyst begins when the follicle doesn't rupture or release its egg, but continues to grow.
- Corpus luteum cyst. When a follicle releases its egg, it begins producing estrogen and progesterone for conception. This follicle is now called the corpus luteum. Sometimes, fluid accumulates inside the follicle, causing the corpus luteum to grow into a cyst.
Functional cysts are usually harmless, rarely cause pain, and often disappear on their own within two or three menstrual cycles.
Ectopic Pregnancy
Ectopic pregnancy occurs when a fertilized egg doesn’t make it to the uterus. Instead, the egg implants in the fallopian tube, and therefore the pregnancy is unable to grow to term.
When the egg continues to grow in the fallopian tube, it will lead to a rupture, severe abdominal or pelvic pain, and heavy internal bleeding. An untreated ectopic pregnancy can be fatal for women.
Tuboovarian Abscess
(TOA) This is a collection of pus in the tubes and ovaries from PID (pelvic inflammatory disease) that is usually accompanied with symptoms of abdominal pain, fever and vaginal discharge. PID is sexually transmitted and can cause infertility. The tuboovarian abscess implies acute infection and therefore requires immediate attention.
Ovarian Cancer and Other Cancers
Ovarian and fallopian tube cancers commonly form a tumor in women that can grow and spread to areas other areas of the body. Common ovarian cancer symptoms include back pain, constipation, heartburn, indigestion, fatigue, irregular periods, difficulty urinating, abdominal or pelvic distension, and painful sex.
Breast and gastrointestinal tract cancers may spread to the adnexal region as well.
Polycystic Ovary
This ovary is enlarged due to the development of many small follicles. Typically, this is seen in women who have polycystic ovarian syndrome (polycystic ovaries, infrequent or lack of menses, and/or evidence of high male hormones).
Endometrioma
Ovarian cyst that contains tissue from the uterine lining or endometrium; also referred to as a “chocolate cyst” because the fluid inside is old blood produced from the endometrial tissue in the cyst and looks like chocolate. This develops as a process of endometriosis.
Dermoid
(aka Mature Cystic Teratoma) This cyst arises in the ovary and is a benign tumor consisting most commonly of hair, fat and teeth. This cyst is common in women between the ages of 20 and 40. If less well-differentiated tissues such as brain, bone, or glands are present then this mass is considered malignant (Immature Teratoma).
Cystadenomas
These develop on the surface of an ovary and might be filled with a watery or a mucous material.
Fibroid
This is a benign tumor of the uterine muscle that may grow adjacent to the uterus, presenting itself in the adnexal region. See website link Fibroids.
Adnexal Cyst and Mass in Pregnancy
To avoid complications, it is ideal to discover an adnexal mass and treat it before a woman gets pregnant. That being said, adnexal masses are sometimes exposed in pregnancy during a routine pelvic exam or ultrasound.
Since most adnexal cysts or masses are not harmful and resolve without treatment, many doctors choose to simply monitor the mass very closely during pregnancy. Women will only require surgery if a complication occurs, the mass is so large that it will likely cause an issue with the pregnancy, or the doctor suspects the adnexal cyst or mass is malignant and therefore may be cancerous.
A clinical review published in OBG Management in 2007 found that about 10% of adnexal masses discovered during pregnancy are considered malignant. However, since the cancer is in often its early stages, this is good news for the mother.
If the malignant tumor is discovered during pregnancy, the doctor will only interfere with a pregnancy if it is no longer safe for the mother.
Risk factors
- Hormonal problems. These include taking the fertility drug clomiphene (Clomid), which is used to cause you to ovulate.
- Pregnancy. Sometimes, the cyst that forms when you ovulate stays on your ovary throughout your pregnancy.
- Endometriosis. This condition causes uterine endometrial cells to grow outside your uterus. Some of the tissue can attach to your ovary and form a growth.
- A severe pelvic infection. If the infection spreads to the ovaries, it can cause cysts.
- A previous ovarian cyst. If you've had one, you're likely to develop more.
Complications
Some women develop less common types of cysts that a doctor finds during a pelvic exam. Cystic ovarian masses that develop after menopause might be cancerous (malignant). That's why it's important to have regular pelvic exams.
Infrequent complications associated with ovarian cysts include:
- Ovarian torsion. Cysts that enlarge can cause the ovary to move, increasing the chance of painful twisting of your ovary (ovarian torsion). Symptoms can include an abrupt onset of severe pelvic pain, nausea and vomiting. Ovarian torsion can also decrease or stop blood flow to the ovaries.
- Rupture. A cyst that ruptures can cause severe pain and internal bleeding. The larger the cyst, the greater the risk of rupture. Vigorous activity that affects the pelvis, such as vaginal intercourse, also increases the risk.
Prevention
Although there's no way to prevent ovarian cysts, regular pelvic examinations help ensure that changes in your ovaries are diagnosed as early as possible. Be alert to changes in your monthly cycle, including unusual menstrual symptoms, especially ones that persist for more than a few cycles. Talk to your doctor about changes that concern you.
How are adnexal masses diagnosed?
The first important step is discussing your medical history with your physician. A family history is also important in determining if you at an increased risk for cancer. Your physician will also ask you about symptoms you may or may not be experiencing to help with the diagnosis, such as abnormal uterine bleeding, weight change, and pain. Next, your physician will perform a physical exam to identify signs of disease. Your physician may be able to palpate the mass and identify from which structure it arises from as well as describe its size, tenderness, consistency, mobility and if it is well-defined or not. The exam is helpful in narrowing down the list of causes so that you do not have to undergo any unnecessary labs or imaging.
One of the most valuable imaging studies we use to identify and characterize adnexal masses is the ultrasound. Adnexal masses on ultrasound have certain characteristics to help your physician identify what type of a mass it is. Blood flow to the ovary can also be visualized on ultrasound, which can help with the diagnosis. Other imaging, such as a CT scan or MRI, may be useful as well.
The main concern with adnexal masses is whether or not they are malignant. A tumor marker called CA-125 is ordered if suspicion for ovarian cancer is high. This tumor marker is not used as a screening tool for ovarian cancer because it can be elevated with many other conditions, such as endometriosis, PID, and fibroids. CA-125 is most useful to follow the levels in those patients already diagnosed with ovarian cancer. There are other tumor markers for different types of ovarian cancers and based on your history, your physician may order some of these as well.
Another important lab test is a pregnancy test to rule out an ectopic pregnancy. Other lab tests may be ordered by your physician to help with making a diagnosis, such as androgen hormone levels to help with the diagnosis of polycystic ovarian syndrome.
How to Treat Adnexal Cyst and Mass
When an adnexal mass or cyst is small and no symptoms are present, treatment may not be required. That being said, your doctor may want to monitor the situation with regular ultrasounds and pelvic exams. In the U.S., a pelvic ultrasonography is considered the most used imaging modality for detecting an adnexal mass.
Surgery is needed when the mass begins to grow, the cyst becomes solid, or the patient develops adnexal cyst symptoms. Adnexal masses that exceed eight centimeters (cm) to 10 cm in size should be managed with a type of abdominal surgery called a laparotomy.
After it is removed, the adnexal cyst or mass will be examined to determine whether the cells within it are cancerous. If cancerous, further treatment may be needed to ensure all the cancer has been removed from the body.
Below is some treatment options of the more common:
- Functional Cysts – Observation is appropriate with serial ultrasounds to make sure that these cysts are not growing or developing concerning features. Some women are just “cyst formers” and birth control pills may be suggested to prevent ovulation and the formation of these cysts. Surgery is recommended to preserve the ovary if the cyst is large enough to undergo torsion.
- Polycystic Ovary – There are no specific treatments for the ovary itself, however women with the syndrome may consider weight loss and birth control pills to help regulate their menstrual cycles. If pregnancy is desired, ovulation induction medications can be used.
- Endometrioma – These cysts usually do not spontaneously regress or respond to medication. Therefore surgery may be recommended for removal.
- Dermoid – Surgery is recommended to prevent growth, torsion, and rupture.
- Fibroma – Since this cyst is prevalent more in postmenopausal women, surgical removal of that ovary and tube is recommended. Preservation of the ovary can also be performed with removal of the fibroma only.
- Cystadenoma – Surgical removal is recommended to prevent growth, torsion, rupture, and rule out malignancy.
- Other benign tumors of the ovary – Surgical removal is recommended to prevent growth, torsion, rupture, and rule out malignancy.
- Tuboovarian Abscess – Hospital admission is required to monitor for signs of the infection spreading to the bloodstream and response to intravenous (IV) antibiotics. Drainage of the abscess may be performed, especially if symptoms do not improve within 24-48 hours. Abscess drainage can be performed under radiologic imaging guidance or can be surgically excised.
- Ectopic Pregnancy – In an asymptomatic patient a medication, called Methotrexate, can be administered in the office with serial ultrasound and lab follow-up until the pregnancy is resorbed. Depending on the severity of the symptoms or characteristic of the ectopic pregnancy, the patient may be a candidate for medical or surgical therapy.
- Hydrosalpinx – If fertility is desired, the tube may need to be surgically repaired or removed. Without fertility desire or symptoms, conservative management may be appropriate.
- Cancer – A referral to an oncologist is strongly recommended for a thorough discussion of the management.
Final Thoughts
An adnexal mass or cyst is often non-cancerous and will resolve without treatment. That being said, when uncomfortable symptoms are experienced, a pelvic exam and ultrasonography may be needed to determine the cause of the adnexal cyst or mass.
Adnexal cyst symptoms are similar to those of many of the potential causes of this condition, including ectopic pregnancy or ovarian cancer. When treated before it spreads outside the ovary, the five-year survival rate of ovarian cancer is considered 92%.
When a liquid-filled cyst becomes solid, surgery may help manage an adnexal cyst or mass. If cancerous, further treatment may be necessary to ensure all cancer has been eliminated from the body.